
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 5
Ileostomy readmission risks: Post-discharge care for patients
James Janez1*; Meghan Varner2; Simon Gelman, PhD3; Arthur Topilow, MD FACP4; Glenn Parker, MD5
1Masters in Biotechnology and a Bachelor’s in Biochemistry and Molecular Biology, Boston University, USA.
2Bachelor of Arts, University of Arkansas 22’, Lincoln Memorial University - DeBusk College of Osteopathic Medicine 28’, USA.
3Research Biostatistician, Office of Research Administration, Hackensack Meridian Health Research Institute, USA.
4Chairman of Hematology/Oncology, retired, Department of Clinical Research, Director of Axelrod Research, Director of Student Programs, USA.
5Vice Chairman of Surgery- Jersey Shore University Medical Center, Chief of Colon and Rectal Surgery- Jersey Shore University Medical Center, President Medical Staff- Jersey Shore University Medical Center, Program Director for General Surgery Residency - Jersey Shore University Medical Center, USA.
*Corresponding Author :Janez James
Masters in Biotechnology and a Bachelor’s in Biochemistry and Molecular Biology, Boston University, USA.
Email: janezj@bu.edu
Received : Mar 04, 2025
Accepted : Apr 09, 2025
Published : Apr 16, 2025
Archived : www.jjgastro.com
Copyright : © James J
Abstract
Ileostomies are complex surgical procedures performed for colonic obstruction or colonic bypass. Postoperative readmission rates among ileostomy patients have become a growing concern, with studies reporting an incidence of approximately 10% to 30%. This prompted a closer examination of causes of and strategies to reduce readmission rates as compared to other surgical procedures. Previous studies have emphasized dehydration as the primary contributor to readmissions and overlooked other contributing factors. With a retrospective review of readmission of ileostomy patient charts, we investigated risk factors contributing to readmission in this population. The findings of this study indicate that in addition to dehydration, readmission rates were significantly influenced by race, diabetes, hypertension, renal problems, Crohn’s disease, cancer, cardiovascular disease, anemia, GERD, diverticulitis, and other comorbidities. This study highlights the critical need for comprehensive assessment and management of post-discharge clinical, and electrolyte-related factors to effectively reduce readmission rates among ileostomy patients, thus contributing to improved patient care and hospital outcomes in this population.
Keywords: Ileostomy; Readmission; Dehydration; Comorbidities; Post-discharge care.
Abbreviations: GERD: Gastroesophageal Reflux Disease; BUN: Blood Urea Nitrogen; CO2: Bicarbonate; Na: Sodium; JSUMC: Jersey Shore University Medical Center; OUMC: Ocean University Medical Center; IRB: Institutional Review Board; K: Potassium; GFR: Glomerular Filtration Rate; BMI: Body Mass Index.
Citation: James J, Varner M, Gelman S, Topilow A, Parker G. Ileostomy readmission risks: Post-discharge care for patients. J Gastroenterol Res Pract. 2025; 5(1): 1226.
Introduction
An ileostomy is a surgical procedure that brings the lumen of the ileum through the abdominal wall through a surgical opening. There are two types of ileostomies: end ileostomy and loop ileostomy both of which can be either temporary or permanent. Ileostomy patients are at an increased risk of postoperative readmission [1]. Ileostomies are essential for patients who experience medical conditions such as colorectal cancer, diverticulitis, Crohn’s disease, ulcerative colitis [2], and other conditions that may impact the function of the colon.
While ileostomies significantly improve patients’ quality of life by restoring bowel function, they can also lead to various complications, which may include stenosis of the bowel, ischemia/necrosis, infection/abscess, electrolyte imbalance due to high effluent output, dehydration, renal impairment, obstruction, fistula formation, and skin irritation [1]. Over recent years, readmission rates due to dehydration have been as high as 10% to 30% in patients who have undergone an ileostomy [3]. The increasing prevalence of postoperative readmissions in ileostomy patients led us to examine the underlying factors contributing to this trend.
Previous studies identified dehydration as the leading cause of readmission in ileostomy patients. Dehydration complicates the effectiveness of an ileostomy and can lead to a long-term impact on renal function and may lead to a significant loss of electrolytes and fluids [4]. Liquid in the intestine is reabsorbed in the colon which is bypassed by an ileostomy. Patients whose ostomy output exceeds 1.5-2 liters in 24 hours are considered to have a high-output stoma and are at a direct risk of dehydration [5]. Ideally, ileostomy outputs should not exceed 1.2 liters of ileostomy output daily [6], and urine specific gravity should be lower than 1.020, indicating the patient is reabsorbing liquids and is not dehydrated [7].
Electrolyte imbalance is often associated with an adverse clinical outcome and an increased risk of readmission among ileostomy patients. Normal electrolyte levels, including Blood Urea Nitrogen (BUN), bicarbonate (CO2), and sodium (Na), play a crucial role in maintaining physiological homeostasis. For instance, the typical range for BUN levels is 5-20 mg/dL, while CO2 levels are expected to be within the range of 21-28 mEq/L, and sodium levels usually range from 137-142 mEq/L [8,9]. Deviations from these established ranges indicate underlying health concerns and could contribute to complications leading to readmission.
While dehydration is reported as a significant contributor to readmission rates among ileostomy patients, analysis of a broader spectrum of risk factors is useful for developing effective preventive strategies. Our aim for this study was to identify the causes of dehydration and examine other risk factors associated with ileostomy. We hypothesize that there is a correlation between the presence of various risk factors and the chance of readmission in ileostomy patients. We analyzed patient records from Jersey Shore University Medical Center (JSUMC) and Ocean University Medical Center (OUMC), to better understand the specific risk factors associated with patients who undergo an ileostomy.
Materials and methods
Our retrospective study involved accessing and analyzing patient records from JSUMC and OUMC for individuals greater than 18 years of age who underwent an ileostomy procedure between January 1, 2019, and December 31, 2022. Patient data was retrieved from the Epic electronic health record system and documented on the RedCap platform to ensure efficient data management and organization. Any patient chart that had incomplete data was excluded from our study. Approval from the hospital IRB was obtained.
Demographic and clinical variables were collected for analysis, including age at the time of the procedure, sex, race, BMI, comorbidities, operative approach, nutritional consultation, patient adherence to nutritional consultation, electrolyte values, bowel antimotility drugs, (and) presence of paralytic ileus, Acute Kidney Injury (AKI), and Chronic Renal Insufficiency (CRI). Electrolyte values were collected for Na, K, CO, BUN, and creatinine levels at the primary discharge and at the Emergency Room (ER) presentation for those who were readmitted.
Patient characteristics of re-admitted and not re-admitted groups were compared with a two-sided Wilcoxon rank sum test, Pearson’s Chi-squared test, or Fisher’s exact test as appropriate. We compared the levels of each electrolyte between discharge and emergency room admission (Table 3). Paired two-sided Wilcoxon rank sum tests were used (Table 4). P-values less than 0.05 were considered significant. Analysis was done with R software (version 4.0.3; packages: ggplot2, ggpubr, and rstatix).
Results
A total of 100 patients underwent ileostomy during the study period. Of these, 65 had complete records and were deemed suitable for analysis. Of the 65 patients, 17(26%) were readmitted within 60 days. Patient demographics and clinical variables between the readmitted and non-readmitted patients were analyzed (Tables 1 & 2).
While there was no statistically significant difference in the mean age at diagnosis between readmitted and non-readmitted patients (p=0.10), a slight trend towards an older age was observed among those readmitted, which could be clinically significant. Gender distribution was insignificant between the two groups (p=0.0522) but a statistically significant difference regarding race was found (p=0.0163), with a higher percentage of black or African American patients among those readmitted. Body Mass Index (BMI) did not differ significantly between the two groups (p=0.351). The distribution of operative approaches (laparoscopic, open, or robotic) did not significantly vary between readmitted and non-readmitted patients (p=0.163). Glomerular Filtration Rate (GFR) analysis at preoperative, postoperative, and readmission stages showed no significant differences between the groups. However, several comorbidities displayed substantial associations with readmission. Readmitted patients exhibited significantly higher rates of diabetes (p=0.0023), hypertension (p<0.0012), renal problems (p=0.0033), Crohn’s disease (p=0.0043), cardiovascular disease (p=0.0153), anemia (p<0.0012), GERD (p<0.0012), and other comorbidities (p=0.0062) compared to non-readmitted patients (Table 1).
Electrolyte levels among ileostomy patients revealed significant differences between discharge and ER. Blood Urea Nitrogen (BUN) levels showed notable elevations between discharge and subsequent ER visits, with a statistically significant p-value of 0.019. Bicarbonate (CO2) levels also had significant variation between visits, with a p-value of 0.014. Creatinine levels showed the most pronounced difference, with a highly significant p-value of 0.000. Potassium (K) levels did not exhibit significant differences between visits, with a p-value of 0.198. Sodium (Na) levels demonstrated significant variation between visits, with a p-value of 0.014. Mean BUN levels at the Emergency Room (ER) visit averaged 33.4 mg/dL, significantly exceeding the normal range of 5-20 mg/dL [8]. Additionally, sodium levels averaged 131.8 milliequivalents per liter (mEq/L), falling below the normal range of 137-142 mEq/L [9] (Tables 3 & 4) (Figure 1).
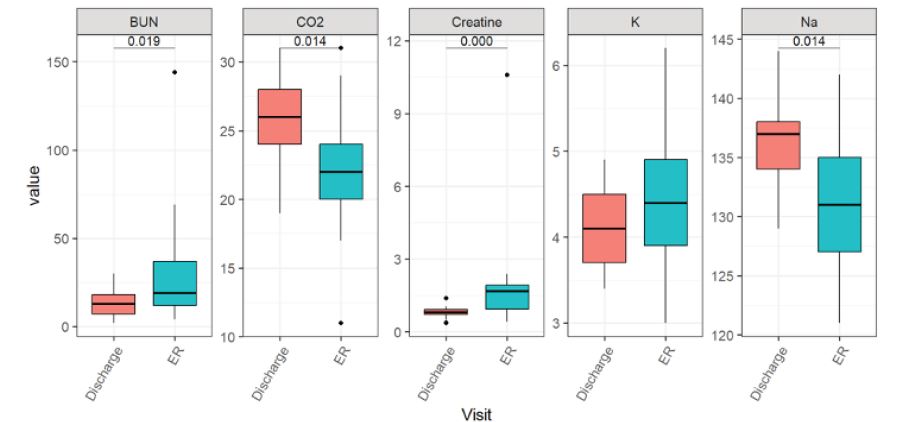
Table 1: Significant clinical factors associated with hospital readmission.
| Characteristic | Overall, N=65 | Not ReadmittedN=48(74%) | Readmitted,N=17(26%) |
|---|---|---|---|
| Race, n (%) | |||
| Asian | 1(1.5) | 0(0) | 1(5.9) |
| Black or African American | 2(3.1) | 0(0) | 2(12) |
| White | 62(95) | 48(100) | 14(82) |
| Renal Problems, n (%) | 13(20) | 5(10) | 8(47) |
| Crohn's Disease, n (%) | 4(6.2) | 0(0) | 4(24) |
| Cardiovascular Disease, n (%) | 10(15) | 4(8.3) | 6(35) |
| Anemia, n (%) | 21(32) | 10(21) | 11(65) |
| GERD, n (%) | 24(37) | 10(21) | 14(82) |
| Diverticulitis, n(%) | 17(26) | 9(19) | 8(47) |
1Wilcoxon rank sum test; 2Pearson’s Chi-squared test; 3Fisher’s exact test; *Number in parenthesis reflects a percentage of the total in that category.
Table 2: Characteristics that showed no bearing on readmission rates.
| Characteristic | Overall, N=65 | Not Readmitted,N=48 (74%) | Readmitted,N=17 (26%) | p-value |
|---|---|---|---|---|
| Cancer, n (%) | 23(35) | 16(33) | 7(41) | 0.562 |
| Age at Diagnosis | 0.101 | |||
| Mean (SD) | 63.3(11.4) | 61.9(11.8) | 67.1(9.6) | |
| Median (IQR) | 63.0(16.0) | 61.5(14.5) | 71.0(13.0) | |
| Range | 37.0-85.0 | 37.0-85.0 | 47.0-80.0 | |
| Sex, n (%) | 0.0522 | |||
| Female | 29(45) | 18(38) | 11(65) | |
| Male | 36(55) | 30(63) | 6(35) | |
| BMI | 0.351 | |||
| Mean (SD) | 30.0(7.1) | 30.3(6.7) | 29.0(8.3) | |
| Median (IQR) | 29.5(10.2) | 30.4(9.0) | 26.3(10.5) | |
| Range | 17.9,48.1 | 17.9,45.0 | 20.3,48.1 | |
| Operative Approach, n (%) | 0.163 | |||
| Laparoscopic | 9(14) | 7(15) | 2(12) | |
| Open | 33(51) | 21(44) | 12(71) | |
| Robotic | 23(35) | 20(42) | 3(18) | |
1Wilcoxon rank sum test; 2Pearson’s Chi-squared test; 3Fisher’s exact test; *Number in parenthesis reflects a percentage of the total in that category.
Table 3: Summary of readmitted patients’ electrolyte levels.
| Discharge | ER | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| BUN | CO2 | Creat. | K | Na | BUN | CO2 | Creat. | K | Na | |
| Value | ||||||||||
| Mean (SD) | 13.3(7.6) | 25.4(3.4) | 0.8(0.2) | 4.1(0.5) | 136.0(3.8) | 33.4(34.6) | 22.0(4.6) | 2.0(2.3) | 4.5(0.8) | 131.8(6.2) |
| Median IQR) | 13.0(11.0) | 26.0(4.0) | 0.8(0.2) | 4.1(0.8) | 137.0(4.0) | 19.0(25.0) | 22.0(4.0) | 1.7(1.0) | 4.4(1.0) | 131.0(8.0) |
| Range | 2.0-30.0 | 19.0-31.0 | 0.4-1.4 | 3.4-4.9 | 129.0-144.0 | 4.0-144.0 | 11.0-31.0 | 0.4-10.6 | 3.0-6.2 | 121.0-142.0 |
Table 4: Comparisons of electrolyte levels between discharge and er among readmitted patients.
| Electrolyte | group1 | group2 | n1 | n2 | p |
|---|---|---|---|---|---|
| BUN | Discharge | ER | 17 | 17 | 0.019 |
| CO2 | Discharge | ER | 17 | 17 | 0.014 |
| Creatine | Discharge | ER | 17 | 17 | 0 |
| K | Discharge | ER | 17 | 17 | 0.198* |
| Na | Discharge | ER | 17 | 17 | 0.014 |
*Showed no significant difference
Discussion
The findings of this study shed light on various factors associated with readmission among ileostomy patients and provide insights into potential areas for clinical intervention and patient-care improvement.
Analysis of patient characteristics revealed several noteworthy trends. Comorbidity analysis revealed significant associations between several medical conditions and readmission risk. Notably, readmitted patients exhibited higher rates of diabetes, hypertension, renal problems, Crohn’s disease, cardiovascular disease, anemia, Gastroesophageal Reflux Disease (GERD), and other comorbidities compared to non-readmitted patients.
Furthermore, the analysis of electrolyte levels at different stages of care revealed significant differences in BUN, CO2, and Na levels between discharge, and Emergency Room (ER) visits. In addition, elevated BUN levels at both discharge and readmission may indicate underlying issues regarding renal function, highlighting the importance of monitoring and managing fluid and electrolyte balance in post-discharge ileostomy patients. Similarly, significant differences in CO2 and Na levels underscore the nature of electrolyte imbalances in this patient population. Specifically, low bicarbonate levels, reflected in CO2 measurements, may indicate metabolic acidosis, potentially contributing to kidney damage if left untreated. Additionally, low sodium levels observed at discharge suggest dehydration, a significant risk factor for readmission in ileostomy patients.
The analysis of blood chemistry values at discharge revealed that all patients were within normal electrolyte ranges. However, upon readmission, average electrolyte levels were found to be out of range for the patients. This suggests that discharge blood values cannot reliably predict the risk of readmission.
While the mean age at diagnosis did not show a statistically significant difference between readmitted and non-readmitted patients, there was a slight trend towards older age among those readmitted. This observation suggests that age may play a role in readmission risk. Additionally, a higher percentage of black or African American patients were observed among those readmitted, indicating a potential racial disparity. It is crucial to acknowledge that the patient population in this study was predominantly white, highlighting the need for future research to encompass a more diverse representation of racial and ethnic backgrounds.
Our findings emphasize the importance of identifying patients with specific risk factors that have previously been shown to contribute to readmission rates. By proactively addressing these factors through targeted interventions, such as additional education, post-discharge support and homecare, our data shows that we can reduce the risk of readmission and improve patient outcomes. Moving forward, efforts should be made to incorporate these insights into discharge planning processes and develop tailored care plans for patients at heightened risk of readmission.
To address the issue of postoperative readmission among ileostomy patients, several potential strategies could be implemented. One approach would be to arrange for weekly follow-up appointments for electrolyte monitoring and management, beginning at the time of ileostomy placement. Incorporating weekly follow-up early in the patient’s care plan may help prevent dehydration and electrolyte imbalance complications. Additionally, there may be a segment of the population that received a nephrology consultation, which may allow a comparison of outcomes between those who did and did not receive specialized follow-up care. Furthermore, educating patients and their families is essential, particularly in cases where ileostomy output exceeds one liter. Families should be advised to contact the surgeon in such instances for timely correction. Another critical factor is outpatient management, as there may be a portion of patients who successfully manage electrolyte correction and hydration without requiring hospital readmission. Understanding who provided this outpatient care—whether it was nephrology, gastroenterology, primary care, or the patient’s family —would be useful for future recommendations. Finally, analyzing the duration of readmission and the specific management strategies employed during these additional hospital stays would offer valuable insight into how to optimize treatment protocols and prevent future readmissions.
Limitations
The limitations of our study include a small patient population, which primarily comprised a single race, raising concerns about the broader applicability of our findings. Additionally, factors like economic status and healthcare accessibility were not thoroughly examined. The retrospective nature of the study and reliance on electronic health record data may introduce biases and limit generalizability.
Future perspective
Future research should aim to establish comprehensive hospital-wide guidelines aimed at preventing readmissions among ileostomy patients. These guidelines should consider the array of risk factors identified in our study and offer interventions to address each patient’s unique needs. Additionally, future researchers should prioritize larger sample sizes and employ multivariate analyses to gain deeper insights into risk factors influencing readmission risk in ileostomy patients.
Conclusion
The study underscores the importance of thorough preoperative assessment, comorbidity management, and home care follow-up along with electrolyte balance monitoring in reducing readmission risk among ileostomy patients. Our analysis also highlights the significance of addressing common risk factors, particularly those prevalent in older patients.
References
- Rajaretnam N, Lieske B. Ileostomy. In StatPearls. StatPearls Publishing. 2023.
- Professional CC. medical. (n.d.). Ileostomy: What it is & when you might need one. Cleveland Clinic. https://my.clevelandclinic.org/health/procedures/21726-ileostomy
- Iqbal A, Sakharuk I, Goldstein L, Tan SA, Qiu P, Li Z, et al. Readmission After Elective Ileostomy in Colorectal Surgery Is Predictable. JSLS: Journal of the Society of Laparoendoscopic Surgeons. 2018; 2: e2018.00008.
- Borucki JP, Schlaeger S, Crane J, Hernon JM, Stearns AT. Risk and consequences of dehydration following colorectal cancer resection with diverting ileostomy. A systematic review and meta-analysis. Colorectal disease: the official journal of the Association of Coloproctology of Great Britain and Ireland. 2021; 23: 1721–1732.
- Workhouse Marketing. Signs of dehydration when you have an ileostomy. Oakmed Healthcare. 2022. https://www.oakmed.co.uk/help-advice/advice-articles/signs-of-dehydration-when-you-have-an-ileostomy/
- Hyperarts RM. (n.d.). Preventing dehydration. Preventing Dehydration | UCSF Ostomy Education Portal. https://ostomy.ucsf.edu/for-patients/ileostomy/preventing-dehydration.aspx#:~:text=No%20more%20than%201200%20ml%20of%20ostomyoutput%20daily.&text=Urine%20should%20be%20a%20light,Actual%20measurements%20are%20important
- Burger M. Metabolic acidosis. StatPearls. 2023. https://www.ncbi.nlm.nih.gov/books/NBK482146/
- Hosten AO. Bun and creatinine. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. 1990. https://www.ncbi.nlm.nih.gov/books/NBK305/
- Ackerman GL. Serum Sodium. In H. K. Walker (Eds.) et al. Clinical Methods: The History, Physical, and Laboratory Examinations. (3rd ed.). Butterworths. 1990.