
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 5
Therapeutic dilemma in ulcerative colitis with coexisting CMV colitis and ischemic stroke
Mansi Hans1; Sunita Aggarwal2*; Pradeep Kumar3; Lochan Gejji1; Ranvijay4; Dheeraj1
1Postgraduate Student, Department of Medicine, Maulana Azad Medical College and Lok Nayak Hospital, India.
2Director & Professor, Department of Medicine, Maulana Azad Medical College and Lok Nayak Hospital, India.
3Professor, Department of Medicine, Maulana Azad Medical College and Lok Nayak Hospital, India.
4Senior Resident, Department of Medicine, Maulana Azad Medical College and Lok Nayak Hospital, India.
*Corresponding Author : Sunita Aggarwal
Director Professor, Mualana Azad Medical College, New Delhi, India.
Email: drsunita.mamc@gmail.com
Received : Jun 03, 2025
Accepted : Jul 07, 2025
Published : Jul 14, 2025
Archived : www.jjgastro.com
Copyright : © Aggarwal S (2025).
Abstract
This case highlights the complex interplay of Ulcerative Colitis (UC), Cytomegalovirus (CMV) colitis, and stroke. It also highlights the challenges of treatment in the context of severe disease activity with per rectal bleeding and thrombotic complications like stroke. A 30-year-old male with severe UC, confirmed by colonoscopy (UCEIS 5/8), was found to have superimposed CMV colitis. Despite treatment with steroids, mesalamine, and ganciclovir, his condition worsened, and he developed an ischemic stroke. Thrombolysis was deferred due to active rectal bleeding, and stroke was managed conservatively. However, the patient ultimately succumbed to his illness. It underscores the importance of a balanced approach to managing these concurrent conditions, considering both the risks and benefits of various therapeutic strategies.
Keywords: Ulcerative colitis; CMV colitis; Stroke; Extraintestinal manifestations; Inflammatory bowel disease.
Citation: Hans M, Aggarwal S, Kumar P, Gejji L, Ranvijay, et al. Therapeutic dilemma in ulcerative colitis with coexisting CMV colitis and ischemic stroke. J Gastroenterol Res Pract. 2025; 5(2): 1231.
Introduction
Ulcerative Colitis (UC) is a chronic inflammatory condition of unknown cause that primarily affects the mucosa of the colon [1]. Approximately 25-40% of UC patient experience extra intestinal manifestations with higher incidence in patients with severe disease activity and long-standing disease, underscoring the systemic inflammatory nature of the condition [2]. It is a prothrombotic state leading to increased risk of stroke which occurs at a frequency of 4.7%. This prothrombotic state is driven by chronic inflammation, endothelial dysfunction, and alterations in the coagulation cascade [3]. The risk can be further worsened in presence of CMV colitis [4]. Cytomegalovirus (CMV) infection typically remains asymptomatic in immunocompetent individuals but can become clinically significant in those with impaired immune function, such as UC patients receiving corticosteroids [5].
Case report
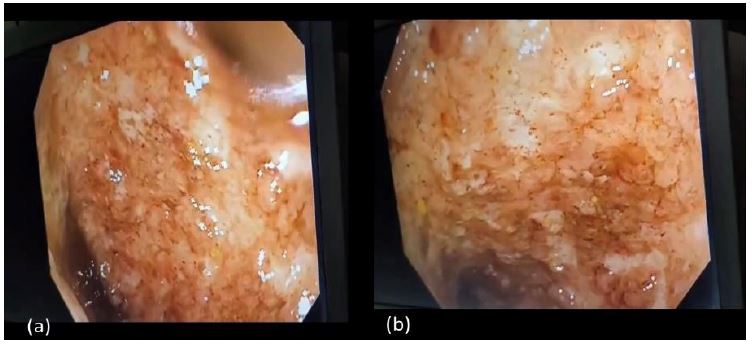
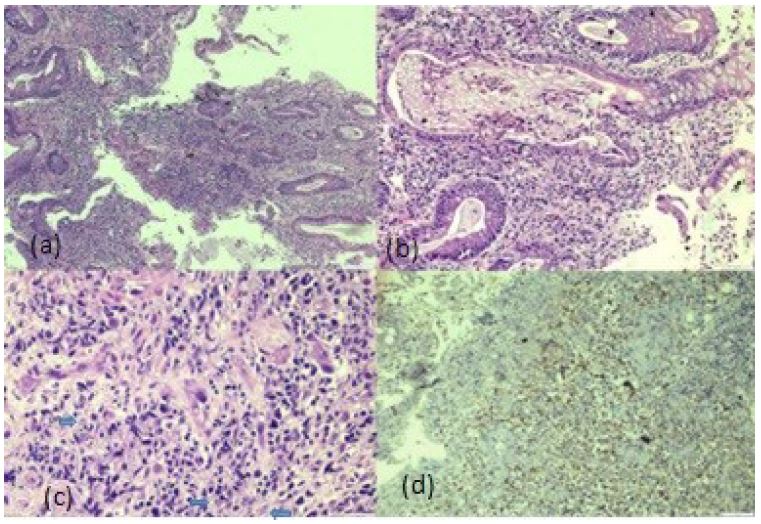
A 30-year-old male with no known comorbidities presented with symptoms suggestive of acute severe UC. He had mild diffuse abdominal tenderness and fresh blood on per rectal examination with no l̥ocal cause (Table 1). Treatment was initiated with intravenous hydrocortisone, oral mesalamine 1.2 gm three times daily, mesalamine suppositories at night. Colonoscopy was consistent with UC (with a UCEIS score of 5/8) with continuous inflammation from the rectum to the transverse colon (Figure 1). A colonic biopsy revealed ulcerative colitis with severe activity and ulceration, with CMV colitis (Figure 2). Serum CMV serology turned out to be positive, with a viral DNA load of 780 IU/mL. Treatment with intravenous ganciclovir 300 mg was started, and steroid therapy was tapered.
Table 1: Routine blood investigations.
| Parameter | Day 2 value | Normal range (Units) |
|---|---|---|
| Hemoglobin (HB) | 8.4 | 13.5–17.5 g/dL |
| Total Leukocyte Count (TLC) | 8210 | 4,000–11,000 /µL |
| Platelet Count (PLT) | 2.34 lakh | 1.5–4.5 lakh/µL |
| Erythrocyte SedimentationRate (ESR) | 48 | <15 mm/hr |
| C-Reactive Protein (CRP) | 73.2 | <5 mg/L |
| Urea | 16 | 10–40 mg/dL |
| Creatinine | 0.8 | 0.6–1.2 mg/dL |
| Sodium (Na) | 136 | 135–145 mmol/L |
| Potassium (K) | 3.4 | 3.5–5.0 mmol/L |
| Procalcitonin (PRO CAL) | 0.172 | <0.1 ng/mL |
| Total Protein (TP) | 4.3 | 6.0–8.0 g/dL |
| Serum Albumin (SA) | 2.2 | 3.4–5.4 g/dL |
| Calcium (CA) | 7.0 | 8.5–10.5 mg/dL |
| Phosphate (PO₄) | 2.0 | 2.5–4.5 mg/dL |
| Total Cholesterol (TC) | 223 | <200 mg/dL |
| Triglycerides (TG) | 176 | <150 mg/dL |
| LDL Cholesterol | 128 | <100 mg/dL |
| HDL Cholesterol | 67 | >40 mg/dL (male) |
| Vitamin D (25-OH) | <7 | 20–50 ng/mL |
| Parathyroid Hormone (PTH) | 61.22 | 10–65 pg/mL |
| PT Activity | 86% | 70–100% |
| INR | 1.05 | 0.8–1.2 |
| Activated Partial Thromboplastin Time (APTT) | 30.1 | 25–35 seconds |
| D-Dimer | 320 | <500 ng/mL |
| HIV | Negative | Negative |
| ANA with pANCA | Negative | Negative |
| cANA | Negative | Negative |
| ASCA | Negative | Negative |
| Stool Routine Microscopy | RBC present,no pus/bacteria | Normally no RBC,pus, or pathogens |
| Clostridium difficile GDH | Negative | Negative |
| Abdominal X-ray | Dilated bowelloop, no air underdiaphragm | no dilation or free air |
HB: Hemoglobin; TLC: Total leucocyte counts; PLT: Platelets; ESR: Erythrocyte sedimentation rate; Na: Sodium; K: Pottasium; Procal: Procalcitonin; CRP: C-reactive protein; TP: Total protein; SA: Serum albumin; CA: Calcium; PO3: Phosphate; TC: Total cholesterol; TG: Triglyceride; LDL: Low density lipid; HDL: High density lipids; VITD: Vitamin D; PTH: Parathyroid; PT activity: Prothrombin activity; INR: International normalised ratio; APTT: Activated partial thromboplastin time; HIV: Human immunodeficiency virus; HEP B: Hepatitis B; HEP C: Hepatitis C; ANA: Antinuclear antibody; pANCA: Perinuclear anti-neutrophilic antibodies; cANCA: Cytoplasmic anti-neutrophilic antibody; ASCA: Anti-saccharomyces cerevisiae antibodies.
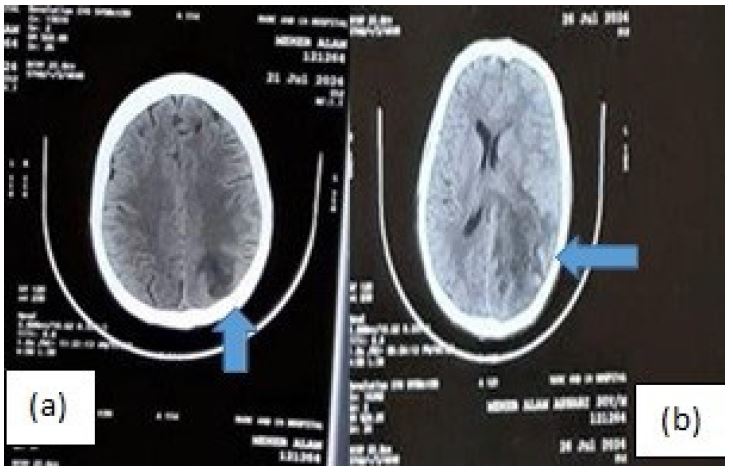
On day 19, the patient developed altered behavior, followed by a Generalized Tonic-Clonic Seizure (GTCS) and was found have developed ischemic infarct with hemorrhagic foci (Figure 3a). A 2D echocardiogram, and lower limb Doppler showed no evidence of thrombus. Following the exclusion of papilledema Cerebrospinal Fluid (CSF) analysis was done which did not reveal any evidence of CMV meningoencephalitis. The patient was managed conservatively with antiedema measures and antiepileptic medication. Subsequently, the patient developed right-sided hemiparesis (NIHSS score of 10), with repeat CT scan showing extension of the infarct with mass effect and a midline shift of 8.7 mm (Figure 3b). Despite maximum medical efforts the patient succumbed to the illness.
Discussion
The incidence of CMV colitis in UC patients ranges from 5-30% in with higher rates observed in patients with severe, steroid-refractory UC [6]. CMV infection is associated with exacerbation of colitis compelling colectomy. Risk factors include age >30 years, immunomodulatory drugs, refractoriness to treatment, leucocyte count <11,000, and disease duration <60 months. Endoscopic findings such as deep ulcers may raise suspicion for CMV, but definitive diagnosis requires histopathological evidence of viral inclusions, immunohistochemistry, or detection of CMV DNA through polymerase chain reaction (PCR) testing of colonic tissue samples [7]. In our patient diagnosis was established with biopsy findings and supported with serum DNA copies. Management was done as per the European Crohn’s and Colitis Organisation (ECCO) and American College of Gastroenterology (ACG) guidelines, which recommend ganciclovir 5 mg/kg twice daily for 2-3 weeks as the first-line agent with valganciclovir as an alternative for less severe cases [8].
According to both guidelines, immunosuppressive therapy should be continued in mild cases of CMV colitis, but in severe cases, particularly steroid-refractory CMV colitis as for our patient, it is recommended to gradually taper steroids as ongoing steroid therapy can worsen CMV colitis, and abrupt cessation can exacerbate UC [9]. Anti-TNF therapy should be considered in cases of CMV- associated acute flare of UC along with antivirals, due to lack of availability at our institution we could not switch to anti-TNF. In cases where medical management fails, colectomy should be considered, particularly in cases of toxic megacolon or perforation.
Our patient further deteriorated with development of ischemic stroke despite prophylactic anticoagulation. Stroke, while a rare but serious complication of UC. The risk of stroke in UC is 1.5-3.6-fold higher as compared to the general population, with a reported frequency of 4.7% [10]. The underlying mechanisms involve multiple factors, including hypercoagulability, chronic inflammation, and endothelial dysfunction. UC is associated with elevated levels of procoagulant factors such as fibrinogen and factor VIII, as well as increased platelet activation and homocysteine levels, all contributing to a prothrombotic state [11]. Ischemic strokes are more common compared to haemorrhagic ones. Vasculitic strokes can occur rarely in the context of severe systemic inflammation. CMV colitis exacerbates the already heightened risk of thrombosis by promoting a pro-inflammatory and hypercoagulable state [12].
Prophylaxis is recommended in patients with active disease or extra-intestinal manifestations, with low-dose aspirin or anticoagulation. While traditional anticoagulants like warfarin have been used, current recommendations often favor direct oral anticoagulants which can also be used on an outpatient basis. Regarding treatment there are no specific guidelines for stroke in context of UC. UC itself is not a contradiction for intravenous thrombolysis but in patients with active bleeding or significant thrombocytopenia, as seen in our patient, intravenous thrombolysis is contraindicated and alternative approaches such as mechanical thrombectomy should be considered which was not available at our facility [13]. Anticoagulation, if required, can be started at lower doses, ensuring that the benefits of preventing further thromboembolic events are weighed against the risk of gastrointestinal bleeding [14].
Several case reports have highlighted the association between acute Cytomegalovirus (CMV) infection and thromboembolic complications, suggesting its potential role as a prothrombotic trigger. Kelkar et al. reported 7 cases of CMV related thromboembolism in patients of renal transplant on immunosuppression even after thromboprophylaxis addressing the association of venous thromboembolic events with CMV [15]. Chou et al. described a patient with CMV colitis who developed pulmonary embolism and management following treatment with intravenous unfractionated heparin and ganciclovir showed clinical improvement [16].
Reinforcing these individual case observations, a nested case-control study by Lee et al., conducted in a Korean cohort of patients with Inflammatory Bowel Disease (IBD), found that CMV colitis was independently associated with an increased risk of Venous Thromboembolism (VTE) (odds ratio 4.01; 95% CI, 1.49- 10.78) [17]. The study also identified elevated C-Reactive Protein (CRP) levels and recent corticosteroid use as additional risk factors, supporting the hypothesis that CMV reactivation can contribute to endothelial injury and a hypercoagulable state. Collectively, these findings underscore the need for heightened vigilance for thromboembolic events in IBD patients with evidence of CMV reactivation. Early initiation of antiviral therapy, alongside appropriate anticoagulation, may be essential for optimizing outcomes in this high-risk population.
Treatment of Ischemic stroke in setting of ulcerative colitis especially when complicated with CMV needs multidisciplinary approach with high clinical suspicion, early diagnosis and prompt treatment to prevent adverse outcomes.
Conclusion
The management of UC and its complications requires a multidisciplinary approach, particularly in the presence of co-existing conditions such as active colitis with bleeding, CMV colitis, and cerebral infarction. In our patient, delayed diagnosis of CMV colitis and absence of thromboembolic prophylaxis in the setting of severe UC led to rapid clinical deterioration and development of an ischemic stroke. Despite appropriate medical therapy, the patient’s condition worsened, and he ultimately succumbed to his illness. Stroke although rare but can occur in UC patients with active colitis and its management particularly in the context of active gastrointestinal bleeding presents significant challenges. Antiviral therapy for CMV colitis and appropriate anticoagulation strategies are essential in improving patient outcomes. Early diagnosis and a tailored treatment plan that addresses both the gastrointestinal and extra-intestinal manifestations of UC are critical for preventing complications and improving prognosis.
References
- Harbord M, Annese V, Vavricka SR, Allez M, Barreiro-de Acosta M, Boberg KM, et al. The first European evidence-based consensus on extra-intestinal manifestations in inflammatory bowel disease. J Crohns Colitis. 2016; 10: 239–54.
- Monsén U, Sorstad J, Hellers G, et al. Extracolonic diagnoses in ulcerative colitis: an epidemiological study. Gut. 1990; 85: 711–6.
- Singh S, Vasudev I, Kerro A, et al. Stroke snapshot: Ulcerative colitis & stroke. Pract Neurol. 2022; 22: 66–7.
- Sherman S, Eytan O, Justo D, et al. Thrombosis associated with acute cytomegalovirus infection: a narrative review. Arch Med Sci. 2014; 6: 1186–90.
- Momayaz Sanat Z, Siami Z, Alatab S, et al. Cytomegalovirus infection in adult patients with inflammatory bowel disease: A literature review. Arch Iran Med. 2024; 27: 277–86.
- Roblin X, Pillet S, Oussalah A, Berthelot P, Del Tedesco E, Phelip JM, et al. Cytomegalovirus load in inflamed intestinal tissue is predictive of resistance to immunosuppressive therapy in ulcerative colitis. Am J Gastroenterol. 2011; 106: 2001–8.
- Cottone M, Pietrosi G, Martorana G, et al. Prevalence of cytomegalovirus infection in severe refractory ulcerative and Crohn’s colitis. Am J Gastroenterol. 2001; 96: 773–5.
- Park SC, Jeen YM, Jeen YT, et al. Approach to cytomegalovirus infections in patients with ulcerative colitis. Korean J Intern Med. 2017; 32: 383–92.
- Rahier JF, Magro F, Abreu C, Armuzzi A, Ben-Horin S, Chowers Y, et al. Second European evidence-based consensus on the prevention, diagnosis and management of opportunistic infections in inflammatory bowel disease. J Crohns Colitis. 2014; 8: 443–68.
- Domènech E, Vega R, Ojanguren I, et al. Cytomegalovirus infection in ulcerative colitis: a prospective, comparative study on prevalence and diagnostic strategy. Inflamm Bowel Dis. 2008; 14: 1373–9.
- Fan JS, Wang M, Chen N, et al. Association between inflammatory bowel disease and risk of stroke: a systematic review and meta-analysis of cohort studies. Front Neurol. 2023; 14: 1204727.
- Wang L, Hsu Y, Sharma N. Thrombosis associated with Cytomegalovirus (CMV) in a kidney transplant recipient. Cureus. 2021; 13: e17745.
- Goh IY, Saric S, Leschke P, et al. Thromboembolism in active ulcerative colitis. BMJ Case Rep. 2017; 2017: bcr-2016-218608.
- Zitomersky NL, Verhave M, Trenor CC. Thrombosis and inflammatory bowel disease: a call for improved awareness and prevention. Inflamm Bowel Dis. 2011; 17: 458–70.
- Kelkar AH, Loc BL, Tarantino M, Rajasekhar A, Wang H, Kelkar M, et al. Cytomegalovirus-associated venous and arterial thrombotic disease. Cureus. 2020; 12: e12161.
- Chou JW, Cheng KS. Pulmonary embolism in an immunocompetent patient with acute cytomegalovirus colitis. Intest Res. 2016; 14: 187–90.
- Lee HS, Kim KJ, Park SH, Yang SK, Kim JM, Choi H, et al. Severe activity and cytomegalovirus colitis may increase risk of venous thromboembolism in inflammatory bowel disease. Gut Liver. 2014; 8: 1032.