
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 5
Aggressive immunosuppression for dermatomyositis gastrointestinal symptoms
Jornod Jennifer A, BMedSci BA1*; Philip Rachel A, High School Diploma2; Peralta Natalie, High School Diploma2; Blount Nicholas J, BS3; Ouellette Taylor J, DO4; Parker Glenn S, MD FACS FASCRS4
1Department of Clinical Studies, St. George’s University School of Medicine, Grenada.
2Axelrod Summer Research Program, Hackensack Meridian Health - Jersey Shore University Medical Center, Grenada.
3Department of Clinical Studies, Hackensack Meridian School of Medicine, Grenada.
4Department of Surgery, Hackensack Meridian Health - Jersey Shore University Medical Center, Grenada.
*Corresponding Author : Jennifer A Jornod
BMedSci, BA, Department of Clinical Studies, St. George’s University School of Medicine, Grenada.
Tel: 407-775-8568;
Email: jjornod@sgu.edu
Received : Sep 04, 2025
Accepted : Oct 21, 2025
Published : Oct 28, 2025
Archived : www.jjgastro.com
Copyright : © Jennifer J (2025).
Abstract
Gastrointestinal involvement of juvenile dermatomyositis is a rare but potentially severe complication, typically attributed to inflammatory injury of the vascular endothelium. We present the case of a 19-year-old male diagnosed with juvenile dermatomyositis with gastrointestinal involvement. Initial studies showed mild duodenitis, multiple ulcers, and edema in the rectosigmoid region. After initiation of an aggressive immunosuppressive regimen, follow-up colonoscopy showed granular mucosa and a diffusely decreased vascular pattern in the rectum, with resolution of prior inflammatory changes. We propose that prompt initiation of aggressive immunosuppressive treatment in young patients with gastrointestinal involvement may reduce long-term colonic complications from inflammation and preserve overall quality of life.
Keywords: Dermatomyositis; Juvenile dermatomyositis; Anti-inflammatory; Immunosuppressive; Gastrointestinal; Colon; Vascular.
Abbreviations: DM: Dermatomyositis; JDM: Juvenile Dermatomyositis; GI: Gastrointestinal; IVIG: Intravenous Immunoglobin; CK: Creatinine Kinase; AST: Aspartate Aminotransferase; ALT: Alanine Aminotransferase; NXP2: Positive Nuclear Matrix Protein 2; CT: Computerized Tomography; MRI: Magnetic Resonance Imaging; IV: Intravenous.
Citation: Jennifer J, Rachel PA, Natalie P, Nicholas BJ, Taylor O, et al. Aggressive immunosuppression for dermatomyositis gastrointestinal symptoms. J Gastroenterol Res Pract. 2025; 5(3): 1235.
Introduction
Dermatomyositis is a rare, idiopathic inflammatory myopathy characterized by progressive proximal muscle weakness and distinctive skin findings such as Gottron’s papules and heliotrope rash [1]. Although the disease most commonly affects skeletal muscle and skin, it can involve other organ systems, including the gastrointestinal tract, particularly in juvenile cases [2]. Juvenile dermatomyositis has an estimated incidence of 2-4 cases per million children annually, and GI complications occur in approximately 22%-37% of the affected patients [3,4]. Though GI manifestations are rare, they are often attributed to immune-mediated small vessel vasculopathy within the GI tract [5]. Damage to capillaries and small arterioles leads to perifascicular muscle fiber atrophy and inflammation, and this vasculopathy may extend beyond muscle tissue, causing ischemic injury in affected organs such as the GI tract [1].
Reported GI complications in dermatomyositis include dysphagia, bowel ulceration or perforation, intestinal pneumatosis, intestinal wall thickening, vasculitis, and vascular ectasia [1]. Symptoms often present acutely or subacutely, with abdominal pain being the most common complaint [1,6]. These complications typically occur during periods of active muscle and skin disease and may develop earlier in juvenile cases than in adults [1]. Early recognition and prompt initiation of aggressive immunosuppressive therapy are essential to disease management. High-dose corticosteroids remain the first-line treatment, often in combination with methotrexate or azathioprine, and surgery may be required for perforation or bleeding [1]. Intravenous immunoglobulin has emerged as an important adjunct therapy in refractory and severe dermatomyositis, including cases with GI involvement, due to its immunomodulatory effects and ability to promote disease remission [7].
In this report, we present a rare case of a 19-year-old male with JDM and early GI involvement, with endoscopic evidence of rectosigmoid ulceration and duodenitis. This case shows the potential benefits of early diagnosis and initiation of aggressive immunosuppressive therapy to control inflammatory progression and achieve resolution of GI involvement and pathology in JDM.
Case presentation
A 19-year-old male presented for a routine follow-up colonoscopy one year after being diagnosed with JDM. His initial symptoms included progressive proximal muscle weakness in all four extremities, arthralgias, dysphagia, decreased appetite, periorbital puffiness, idiopathic urticaria across multiple body areas, and a questionable history of a photosensitive, pale pink forehead rash. Upon physical examination, he was noted to have abdominal and muscle tenderness, mild hepatosplenomegaly, and motor weakness on neurological examination.
Initial laboratory studies were notable for elevated muscle enzymes and inflammatory markers, including creatine kinase, aldolase, aspartate aminotransferase, alanine aminotransferase, lactate dehydrogenase, and erythrocyte sediment rate. Autoimmune workup revealed a positive antinuclear antibody with a speckled nuclear pattern and elevated titer, as well as positive nuclear matrix protein 2 antibodies. Additional findings included elevated von Willebrand factor, neutrophilia, monocytosis, and lymphopenia. MRI of the femurs showed symmetric bilateral myositis, and MRI of the pelvis demonstrated systemic myositis involving bilateral pelvic and visualized muscles. The diagnosis of JDM was confirmed by muscle and nerve biopsy. Initial CT imaging of the abdomen revealed sigmoid colon wall thickening, raising suspicion for malignancy. Upper endoscopy at diagnosis showed three superficial duodenal ulcers and chronic duodenitis. Colonoscopy at that time demonstrated edema and ulceration in the rectosigmoid region (Figure 1).
Following diagnosis, the patient was treated with oral prednisone, hydroxychloroquine, and methotrexate, along with IV methylprednisolone. A follow-up MRI of the abdomen and pelvis four months later showed persistent colonic changes at the rectosigmoid junction, along with distal proctitis. IVIG was initiated four months after diagnosis due to insurance delays. Treatment began with IVIG 70 g once every two weeks for three doses, then transitioned to monthly infusions. Methylprednisolone 1 g was administered concurrently with the first three doses. The IVIG interval was subsequently extended from biweekly to every four weeks, and then every six weeks.
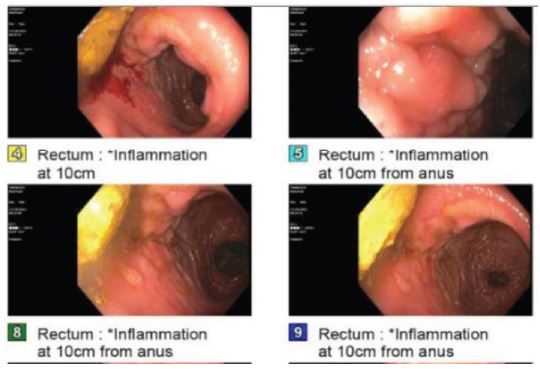
Fifteen months after diagnosis, a repeat colonoscopy revealed a diffuse area of granular rectal mucosa with decreased mucosal vascularity and resolution of ulcerations (Figure 2). A biopsy of the rectal wall showed resolution of ulcerations, evidence of improved mucosal healing and mild chronic inflammatory changes. During the procedure, a colonic stricture was identified and managed with balloon dilation.
At present, the patient continues treatment with high-dose corticosteroids, methotrexate, hydroxychloroquine, and IVIG infusions every ten weeks. His laboratory results show normalization of CK and aldolase levels, while ALT and AST levels remain elevated. During follow-up, the patient experienced improvement in bowel function and nutrition status. At 15 months post-diagnosis, the disease remains stable with ongoing clinical monitoring occurring at three-month intervals.

Discussion
Dermatomyositis rarely involves gastrointestinal manifestations such as ulceration, intestinal pneumatosis, and vasculitis. However, patients diagnosed with JDM and NXP2 antibodies are at a higher risk for GI complications that are associated with poor outcomes and high mortality rates [8]. Our patient presented with GI involvement early in his disease course, which has allowed us to compare the colonoscopy findings following treatment with pre-treatment findings (Figure 1 & 2). The resolution of the rectal ulceration and proctitis on follow-up colonoscopy along with the normal CK and aldolase levels suggest that aggressive immunosuppressive therapy is promising with regard to controlling GI disease progression and preventing additional colonic complications of JDM. The decreased vascular pattern, however, poses an increased risk of recurrent proctitis in addition to the increased risk of recurrent GI involvement from his JDM.
Our patient’s early GI involvement and severity of symptoms were indicative of more severe JDM which necessitated the aggressiveness of the treatment regimen. Patients diagnosed with JDM and GI involvement have previously been reported to be treated with corticosteroids, methylprednisolone pulses, rituximab, intravenous immunoglobulin, cyclophosphamide, methotrexate, cyclosporine A, mycophenolate mofetil, and other traditional disease-modifying anti-rheumatic drugs [1,2,5,7,8]. Our patient was treated with oral prednisone, hydroxychloroquine, and methotrexate, along with IVIG and IV methylprednisolone. This combination of medications targets multiple inflammatory pathways. By reducing the overall production of pro-inflammatory substances, the vasculature of the colonic wall remains intact, thereby reducing the risk of continued edema and colonic ulceration.
Since 77% of gastrointestinal perforations occur within one year of JDM presentation [6], the resolution of colonic edema and ulceration in our patient points to the effectiveness of early and aggressive anti-inflammatory treatment for GI manifestations of JDM. Early diagnosis of gastrointestinal symptoms after diagnosis and prompt initiation of aggressive anti-inflammatory treatment will improve the effectiveness of treatment regimens by reducing the amount of tissue damage sustained.
Overall, our patient was treated aggressively for severe JDM, which might be key in combating the early GI findings. Initiating an early, aggressive immunosuppressive regimen shows promise for reducing morbidity and mortality in patients with GI involvement in JDM. Comparative studies of various aggressive immunosuppressive regimens are still needed to optimize treatment of GI involvement in JDM. We suggest that strong immunosuppressive regimens with anti-inflammatory properties for patients with gastrointestinal involvement in juvenile dermatomyositis could reduce long-term colonic complications and preserve quality of life.
Conclusion
Early gastrointestinal involvement allowed comparative assessment of pre- and post-treatment findings in this patient. Resolution of rectal ulceration suggests that aggressive immunosuppressive therapy effectively controls disease progression. However, reduced vascularity poses an ongoing risk of recurrent proctitis and gastrointestinal complications. This case shows the potential benefit of early, aggressive immunosuppressive therapy in mitigating gastrointestinal complications of juvenile dermatomyositis.
Declarations
Conflicts of interest: The authors have no conflicts of interest to declare.
Funding sources: This study was not supported by any sponsor or fund.
Acknowledgements: We would like to thank Hackensack Meridian Health – Jersey Shore University Medical Center for the opportunity to train and research at their institution.
Funding: No funding was received for this project.
References
- Matas-Garcia A, Milisenda JC, Espinosa G, et al. Gastrointestinal involvement in dermatomyositis. Diagnostics. 2022; 12: 1200.
- Rider LG, Katz JD, Jones OY. Developments in the classification and treatment of the juvenile idiopathic inflammatory myopathies. Rheum Dis Clin North Am. 2013; 39: 877-904.
- Besnard C, Gitiaux C, Girard M, et al. Severe abdominal manifestations in juvenile dermatomyositis. J Pediatr Gastroenterol Nutr. 2020; 70: 247-51.
- Kwa MC, Silverberg JI, Ardalan K. Inpatient burden of juvenile dermatomyositis among children in the United States. Pediatr Rheumatol. 2018; 16: 70.
- Papadopoulou C, Wedderburn LR. Treatment of juvenile dermatomyositis: an update. Paediatr Drugs. 2017; 19: 423-34.
- Xu X, Ye S, Jin Y, et al. Anti-nuclear matrix protein 2 antibody-associated juvenile dermatomyositis with gastrointestinal perforations successfully treated with traditional therapeutic drugs combined with vedolizumab: a case report and literature review. Front Pediatr. 2025; 12: 1522559.
- Marie I, Levesque H, Cailleux N, Courtois H, Guédon C. Intravenous immunoglobulin for treatment of gastrointestinal haemorrhage in dermatomyositis. Ann Rheum Dis. 2001; 60: 723-4.
- Xiangyuan C, Xiaoling Z, Guangchao S, Huasong Z, Dexin L. Juvenile dermatomyositis complications: navigating gastrointestinal perforations and treatment challenges, a case report. Front Pediatr. 2024; 12: 1419355.